Epidemiology of Acute Kidney Injury
- Recent surveys demonstrated that the worldwide incidence of acute kidney injury (AKI) is increasing, occurring in 21% of hospital admissions.
- Several risk factors for AKI development have been highlighted recently, such as fluid overload, chloride-rich intravenous fluid therapy, anemia, hyperuricemia, and use of warfarin.
- New biomarkers of kidney injury, such as urinary neutrophil gelatinase-associated lipocalin, cystatin C, and interleukin-18, have been able to identify patients with AKI who present the worse prognosis, particularly critically ill patients.
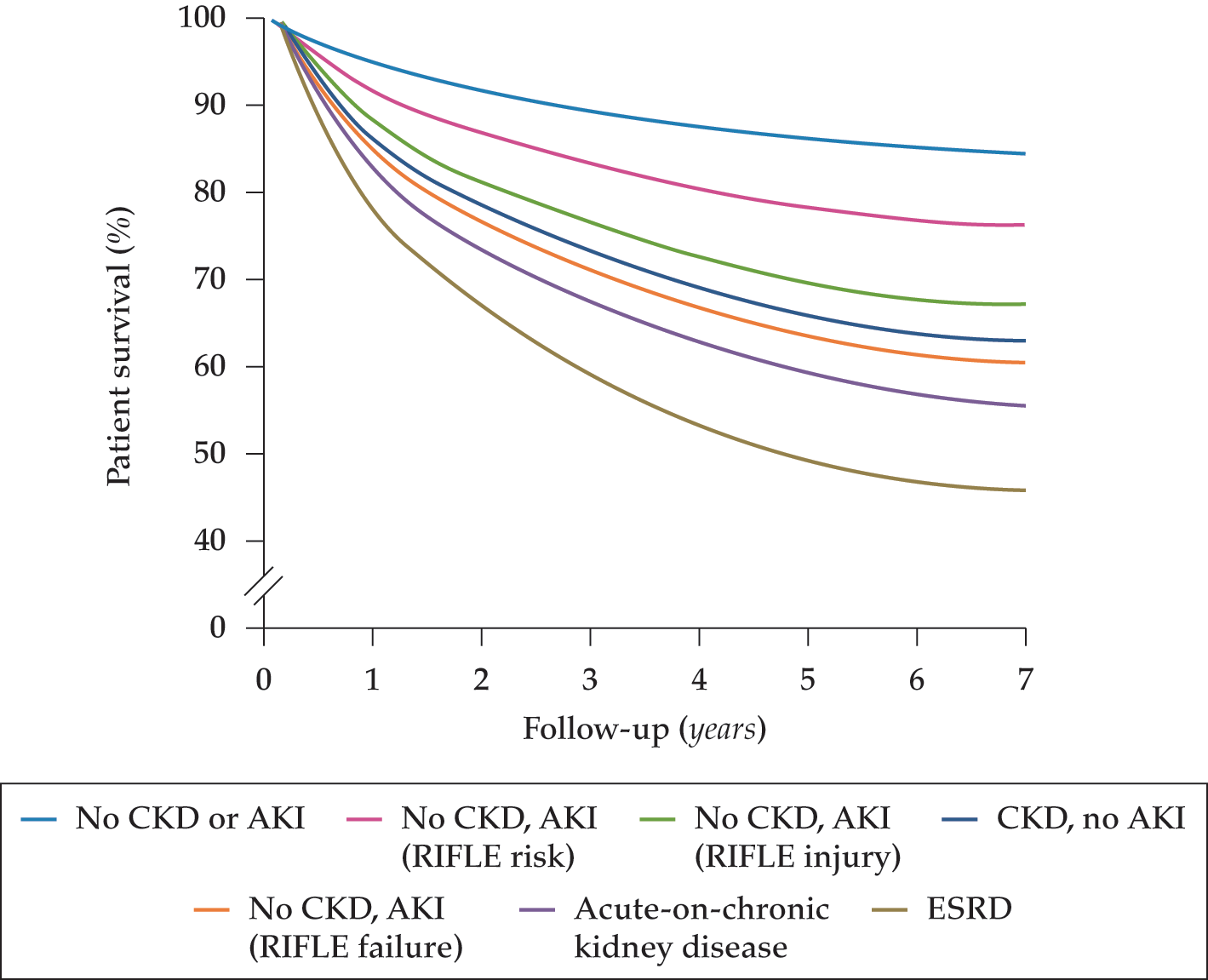
- Hospital-associated AKI is associated with long-term mortality, and the most important risk factors for this late lethality are older age, preexisting comorbid disease (chronic kidney disease [CKD], cardiovascular disease, or malignancy), and incomplete organ recovery with persistent kidney damage.
- AKI is associated with de novo end-stage renal disease (ESRD) (CKD development, progression of preexisting CKD) and the occurrence of ESRD in the long term, and high-risk patients recovering from an AKI episode such as those with baseline CKD, diabetes mellitus, or heart failure and those dialyzed for AKI should likely be followed by a nephrologist.










.png)