- Breast sarcomas are typically larger than adenocarcinomas and grow rapidly
- Skin changes suggest angiosarcoma, and punch biopsy is diagnostic
- Mastectomy is recommended in most cases
- Routine nodal sampling is not recommended
- Five-year survival for breast sarcoma is 60%
Latest Updates


- The incidence of Paget disease (PD) associated with an underlying invasive and/or noninvasive cancer is decreasing, whereas the incidence of PD identified without an associated underlying cancer has remained stable.
- Breast MRI is an effective method to screen the breast when PD is identified in the setting of an otherwise negative mammogram.
- Mastectomy has been the historical gold standard for treatment of PD; however, the use of breast-conserving surgery is on the rise and appropriate in many cases.
- Sentinel node biopsy is feasible in patients with PD and should be used in those presenting with PD and an underlying invasive carcinoma. Its use in patients with PD with ductal carcinoma in situ or PD alone is controversial.
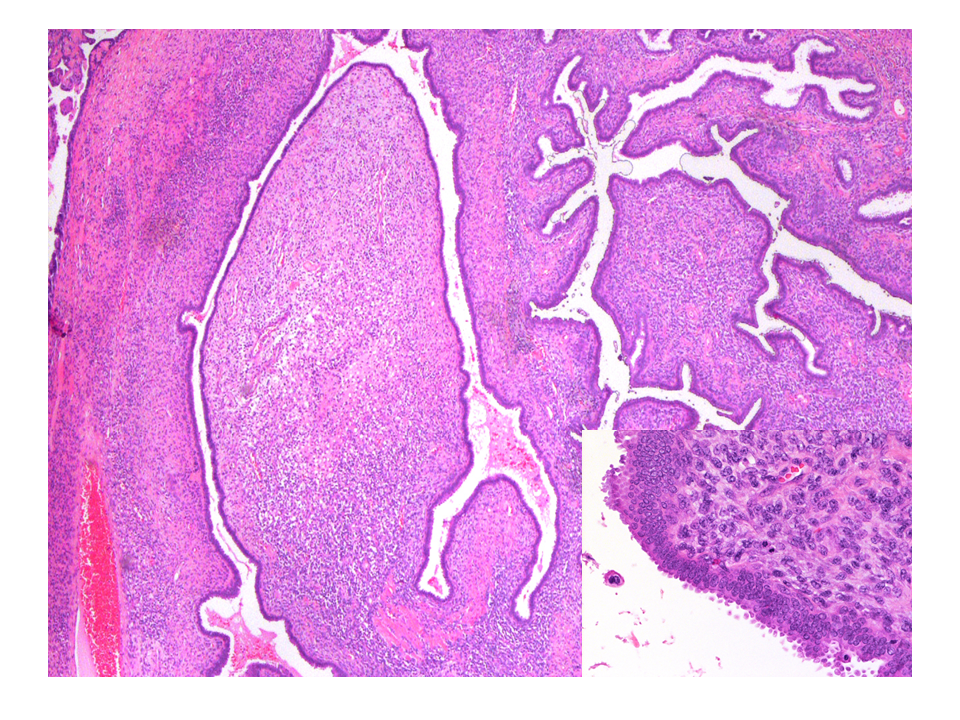
Breast Cancers: Phyllodes Tumors
- Percutaneous core-needle biopsy is recommended as the first step in diagnosis of breast lesions suspicious for phyllodes tumors, and surgical excisional biopsy is recommended for a core-needle biopsy diagnosis of cellular fibroepithelial lesion or a lesion suspicious for phyllodes tumor.
- Surgical treatment parallels that for soft tissue sarcoma rather than breast adenocarcinoma. Wide local excision and mastectomy with 1 cm tumor-free margins are equally appropriate treatments for phyllodes tumors, the choice of which should be governed by tumor size in relation to breast size, anticipated cosmesis, and patient preference. Tumor enucleation, subtotal resection, and positive final margins should be avoided.
- Axillary staging or dissection is not recommended.
- Adjuvant radiation is not recommended as routine, nor is adjuvant chemotherapy.
- Molecular genetic analyses of phyllodes tumors recently have identified potentially targetable mutations that may, in the future, guide therapy for high-risk, recurrent, or metastatic phyllodes tumors.

Breast Cancers: Paget Disease of the Breast
- The incidence of Paget disease (PD) associated with an underlying invasive and/or noninvasive cancer is decreasing, whereas the incidence of PD identified without an associated underlying cancer has remained stable.
- Breast MRI is an effective method to screen the breast when PD is identified in the setting of an otherwise negative mammogram.
- Mastectomy has been the historical gold standard for treatment of PD; however, the use of breast-conserving surgery is on the rise and appropriate in many cases.
- Sentinel node biopsy is feasible in patients with PD and should be used in those presenting with PD and an underlying invasive carcinoma. Its use in patients with PD with ductal carcinoma in situ or PD alone is controversial.

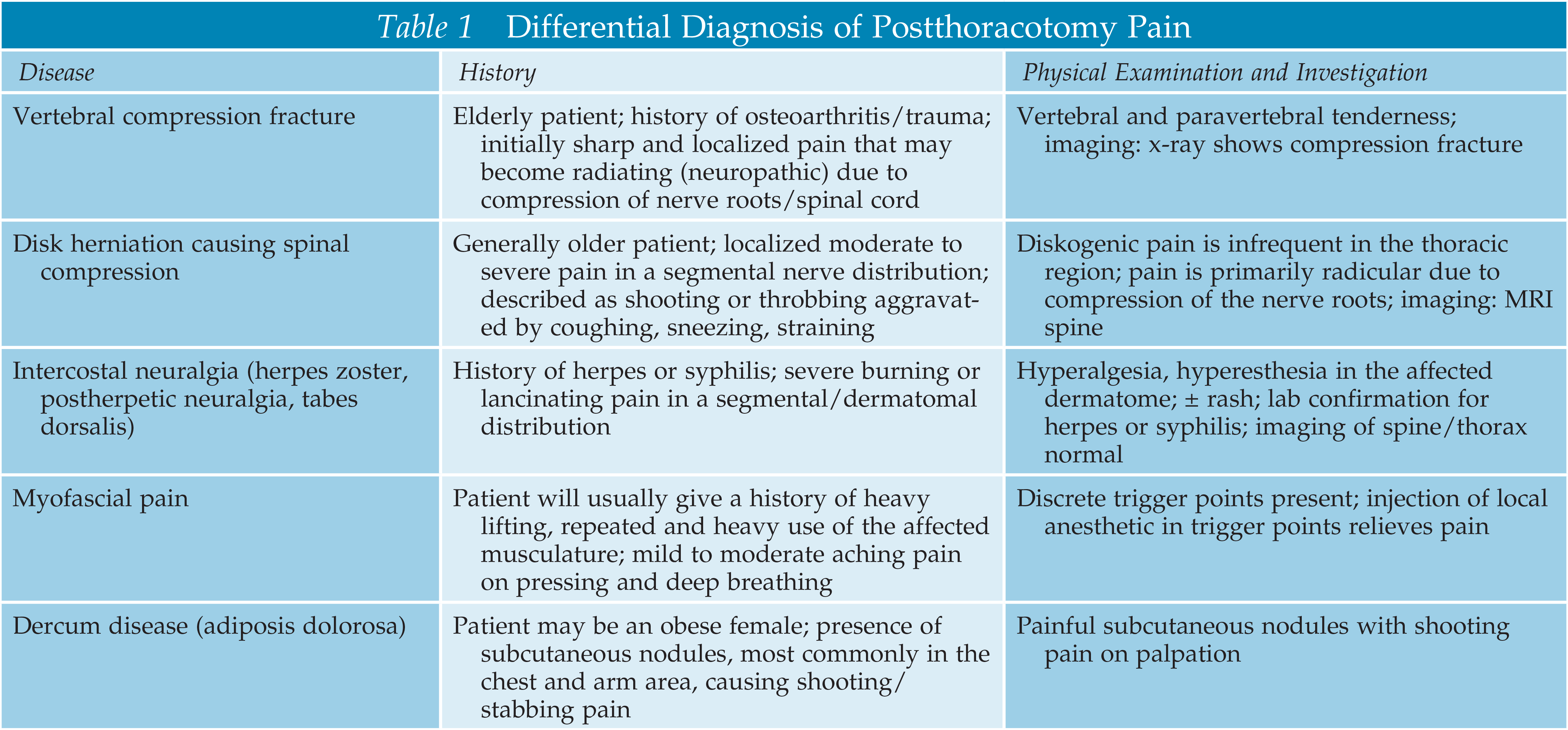
Pain Related Disease States: Patient with Postthoracotomy Pain
- Recent randomized controlled trials (RCTs) demonstrated that surgical techniques can be a significant factor in the development of chronic postthoracotomy pain (CPTP) syndrome. CPTP was significantly less common and had a lower chance of being neuropathic with video-assisted thoracoscopic surgery (VATS) compared with open thoracotomy surgery. Furthermore, outcomes were significantly better when the thoracotomy wounds were closed using a subcostal closure technique compared with VATS. In addition to peripheral nerve factors, animal studies demonstrated that neurokinin-1 receptor–expressing neurons in the rostral ventromedial medulla appear to be essential for the development of CPTP.
- Recent systematic reviews concluded that thoracic paravertebral block seems as effective as thoracic epidural analgesia (TEA) for postthoracotomy pain relief but is associated with fewer complications. A more recent RCT demonstrated that ultrasonography-guided serratus anterior plane block can be an alternative to TEA, with improved perioperative hemodynamic outcomes.
- Recent RCTs provided evidence of two effective measures to reduce the risk of developing CPTP. Preoperatively initiated TEA was associated with better pain control and decreased incidence (and intensity) of CPTP compared with postoperative (epidural or intravenous) analgesia. Total intravenous anesthesia significantly reduced the incidence of CPTP compared with inhalation anesthesia. In contrast, intravenous or epidural ketamine administration failed to reduce CPTP.
- In an RCT, a pregabalin-methylcobalamin combination was shown to be safe and effective in the treatment of CPTP, with minimal side effects.
- Percutaneous core-needle biopsy is recommended as the first step in diagnosis of breast lesions suspicious for phyllodes tumors, and surgical excisional biopsy is recommended for a core-needle biopsy diagnosis of cellular fibroepithelial lesion or a lesion suspicious for phyllodes tumor.
- Surgical treatment parallels that for soft tissue sarcoma rather than breast adenocarcinoma. Wide local excision and mastectomy with 1 cm tumor-free margins are equally appropriate treatments for phyllodes tumors, the choice of which should be governed by tumor size in relation to breast size, anticipated cosmesis, and patient preference. Tumor enucleation, subtotal resection, and positive final margins should be avoided.
- Axillary staging or dissection is not recommended.
- Adjuvant radiation is not recommended as routine, nor is adjuvant chemotherapy.
- Molecular genetic analyses of phyllodes tumors recently have identified potentially targetable mutations that may, in the future, guide therapy for high-risk, recurrent, or metastatic phyllodes tumors.

Skin Cancers: Basal Cell Carcinoma: Epidemiology, Risk Factors, and Treatment Options
- Risk factors for patients at risk for developing basal cell skin cancers (BCCs) include exposure to UV solar radiation, long-term immunosuppression, exposure to ionizing radiation, and certain genetic disorders.
- Treatment modalities can be divided into surgical and nonsurgical therapies, although surgical therapy is generally the mainstay of treatment.
- Superficial therapies, such as topical imiquimod or 5-fluorouracil, photodynamic therapy, or cryotherapy, may be effective for anatomically challenging locations where surgery or radiation is contraindicated, but the cure rates of these approaches are lower compared with surgery.
- Recent FDA-approved hedgehog pathway inhibitors include vismodegib and sonidegib for patients who have exhausted surgical and radiation options for treating advanced BCC.

Breast Cancers: High-Risk Breast Lesions
- Atypical ductal hyperplasia diagnosed on core biopsy requires excision because of the risk of cancer present at the site, but expert histologic review may be helpful because of the risk of misdiagnosis.
- Pleomorphic lobular carcinoma in situ should be treated as ductal carcinoma in situ based on its behavior and greater risk of associated invasive disease.
- Excision of pseudoangiomatous stromal hyperplasia has been questioned because of limited data suggesting that imaging discordance and the presence of suspicious clinical findings are the primary risk factors for associated cancer, and their absence may permit safe observation.








.png)