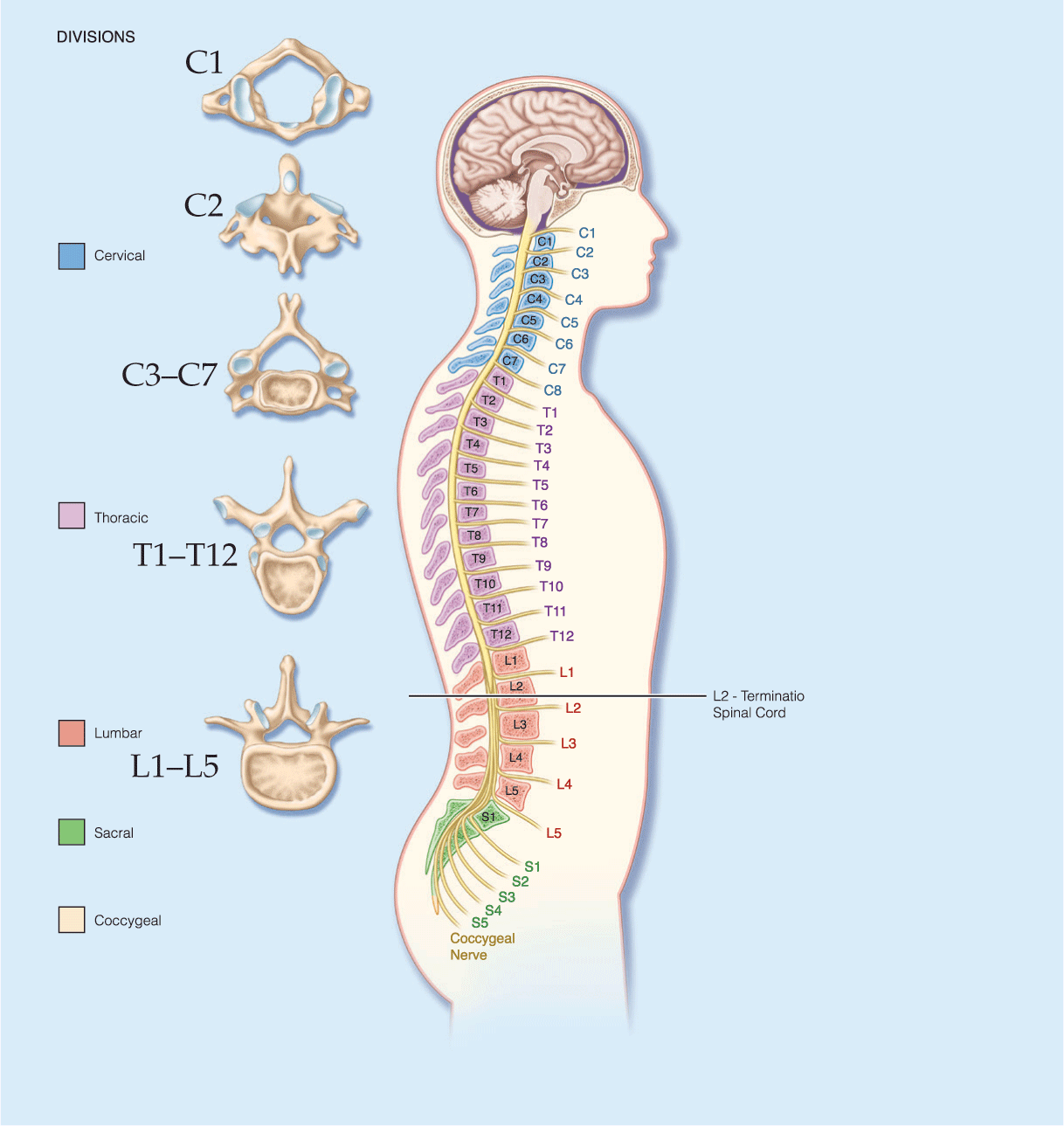
- Blood pressure management is essential in spinal injury management: IV Crystalloid, blood products and/or norepinephrine should be used to maintain SBP >90 mmHg and MAP between 85-90 mm Hg
- Intravenous steroid administration may be considered in the first 8 hours after blunt spinal cord injury in consultation with a spinal specialist and with patient and/or family understanding the risks and benefits.
- If required, surgical intervention within 24 hours of injury is associated with improved long-term outcomes in spinal cord injury.
Latest Updates


- Response to chemoradiation should be assessed for up to 26 weeks, provided there is no evidence of progression.
- Varying regimens for chemoradiation, including capecitabine, as an alternative to 5-fluorouracil and the introduction of intensity-modulated radiation therapy
- Nivolumab as a potential second- or third-line treatment in refractory metastatic squamous cell carcinoma

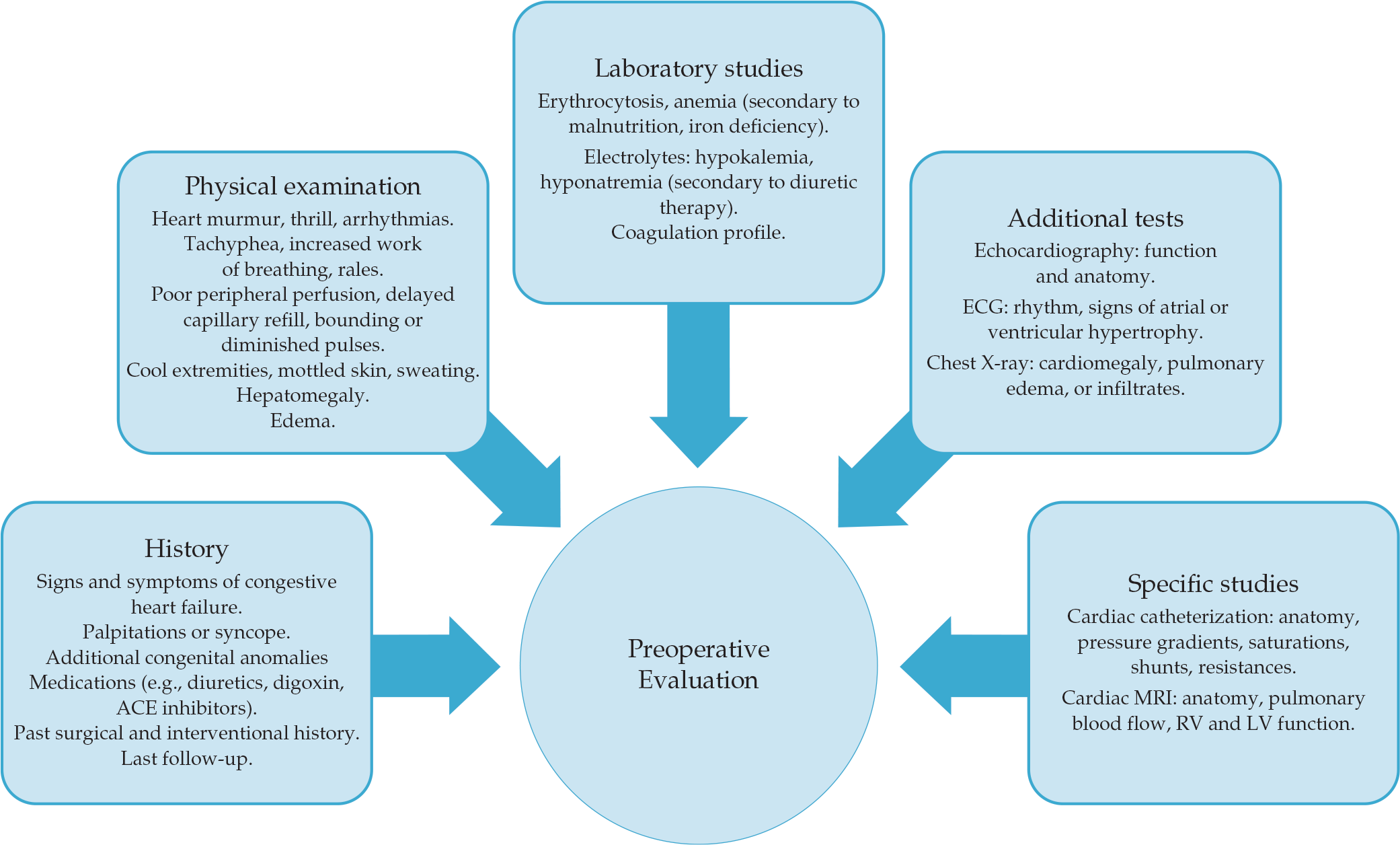
Anesthesia for Common Cardiac Lesions
- Management of cardiopulmonary bypass has improved with ultrafiltration.
- Neuromonitoring including cerebral oximetry is becoming routine in cardiac surgery.
- Transesophageal echocardiography is a great tool for the diagnosis and evaluation of pre- and post- surgical procedures.
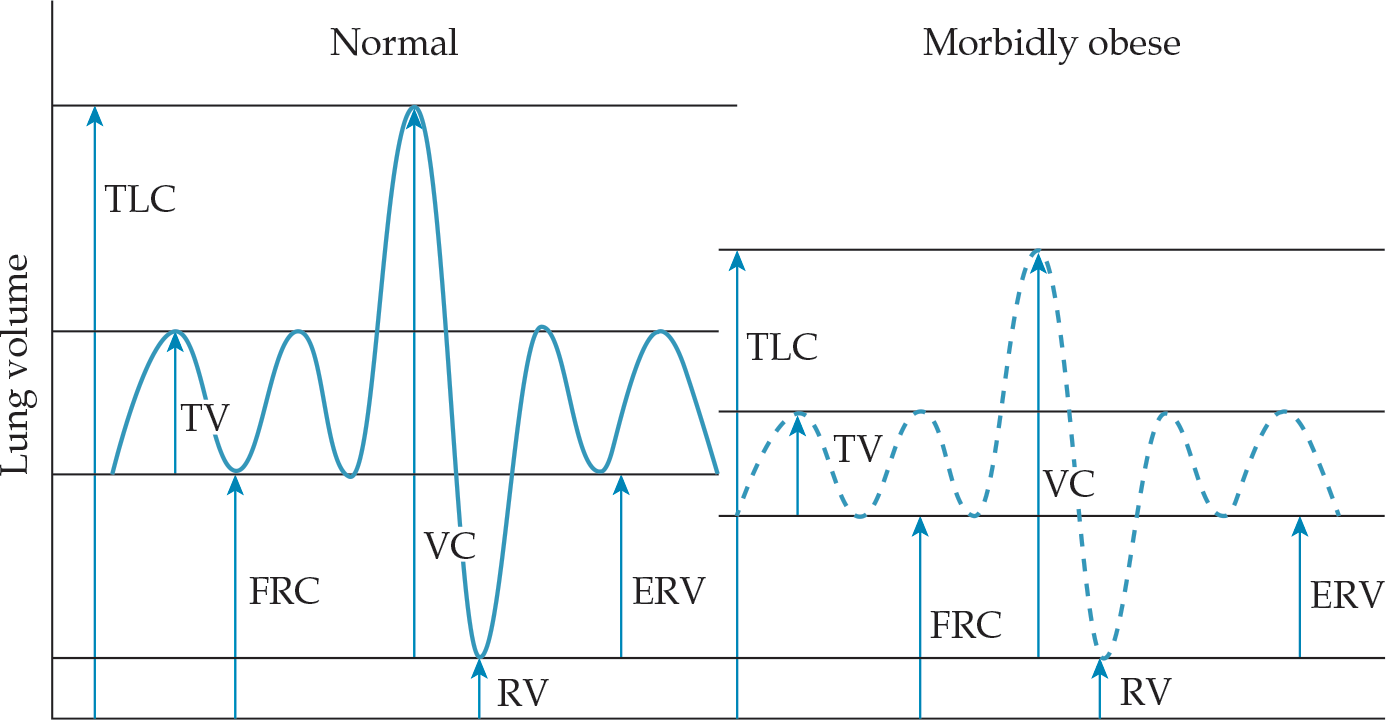
- The use of suggamadex versus traditional neuromuscular blockade reversal may lead to improved postoperative pulmonary outcomes in obese patients.
- The advent and use of less fat-soluble volatile anesthetics, such as desflurane, leads to faster emergence and return of airway reflexes and may improve postoperative pulmonary outcomes in the obese patient.
- Creation of obesity-specific perioperative guidelines from the Society of Bariatric Anesthesia
- Creation of specific operative equipment to assist with the transportation and positioning of obese patients

- Blood pressure management is essential in spinal injury management: IV Crystalloid, blood products and/or norepinephrine should be used to maintain SBP >90 mmHg and MAP between 85-90 mm Hg
- Intravenous steroid administration may be considered in the first 8 hours after blunt spinal cord injury in consultation with a spinal specialist and with patient and/or family understanding the risks and benefits.
- If required, surgical intervention within 24 hours of injury is associated with improved long-term outcomes in spinal cord injury.

- Response to chemoradiation should be assessed for up to 26 weeks, provided there is no evidence of progression.
- Varying regimens for chemoradiation, including capecitabine, as an alternative to 5-fluorouracil and the introduction of intensity-modulated radiation therapy
- Nivolumab as a potential second- or third-line treatment in refractory metastatic squamous cell carcinoma
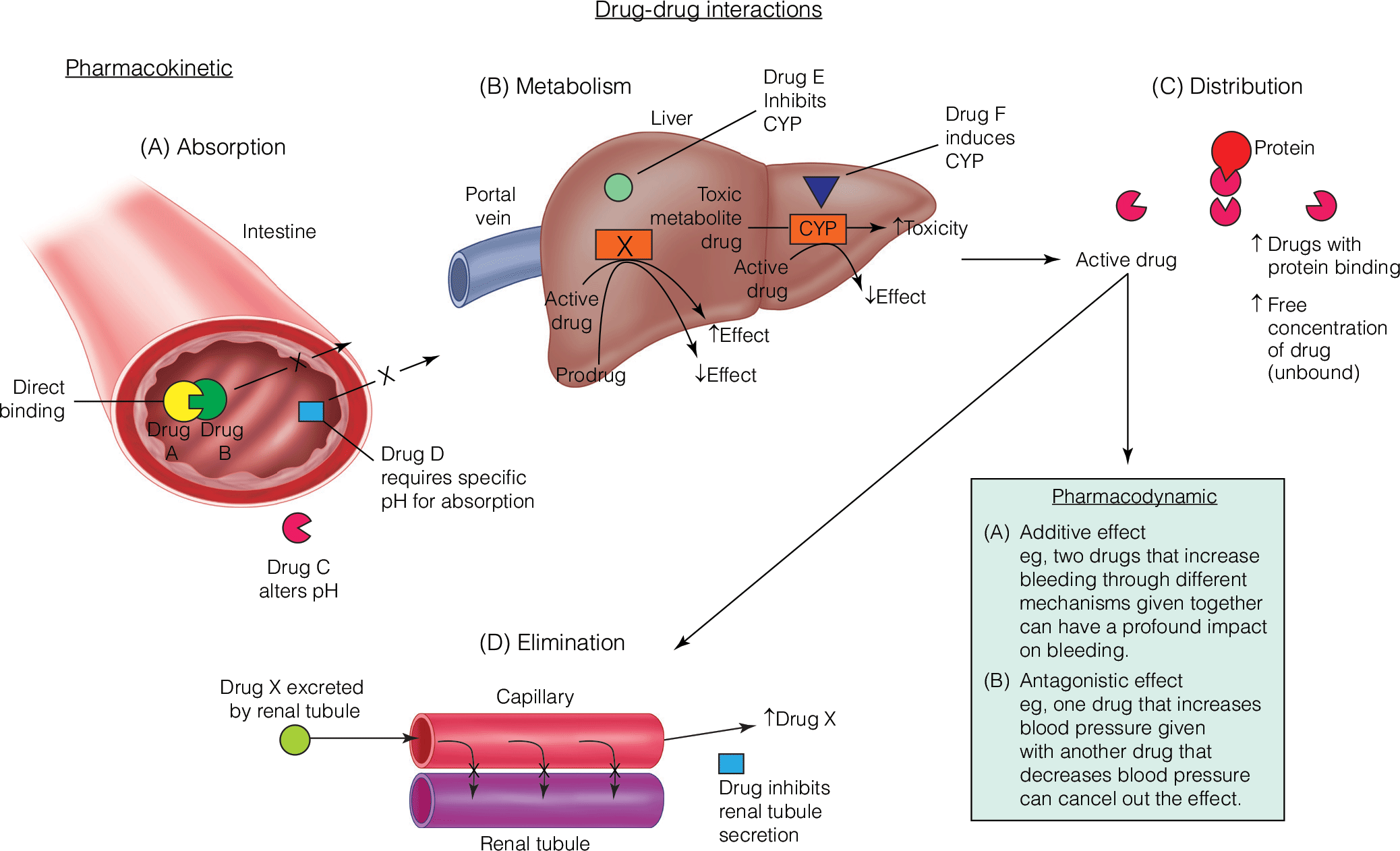
Management of Drug Interactions between Anti-infective and Common Anesthetics
- Rocuronium-induced neuromuscular blockade is potentiated by a synergistic effect of gentamicin and clindamycin, which may delay recovery.
- Penicillins form a complex with sugammadex, which may interfere with the therapeutically intended sugammadex-rocuronium complex.
- Ondansetron can decrease the analgesic efficacy of acetaminophen at high doses.
- Anesthesiologists are positioned to manage interactions between anesthetic agents and antimicrobials in the operating room.

- Maintain a mean arterial blood pressure 85-90 mmHg for 7 days following injury.
- Methylprednisolone is not recommended for treatment of traumatic spinal cord injury.
- Obtain MRI if incomplete neurologic deficit or findings that do not correlate with CT.





.png)