- Compartment syndrome of the extremity is a clinical diagnosis in an awake and alert patient.
- Measurement of intracompartmental pressures should be performed in the obtunded patient or if clinical assessment is inconclusive.
- Once the diagnosis is made, emergent fasciotomy is the treatment of choice as time to fasciotomy is the most important factor determining outcome.
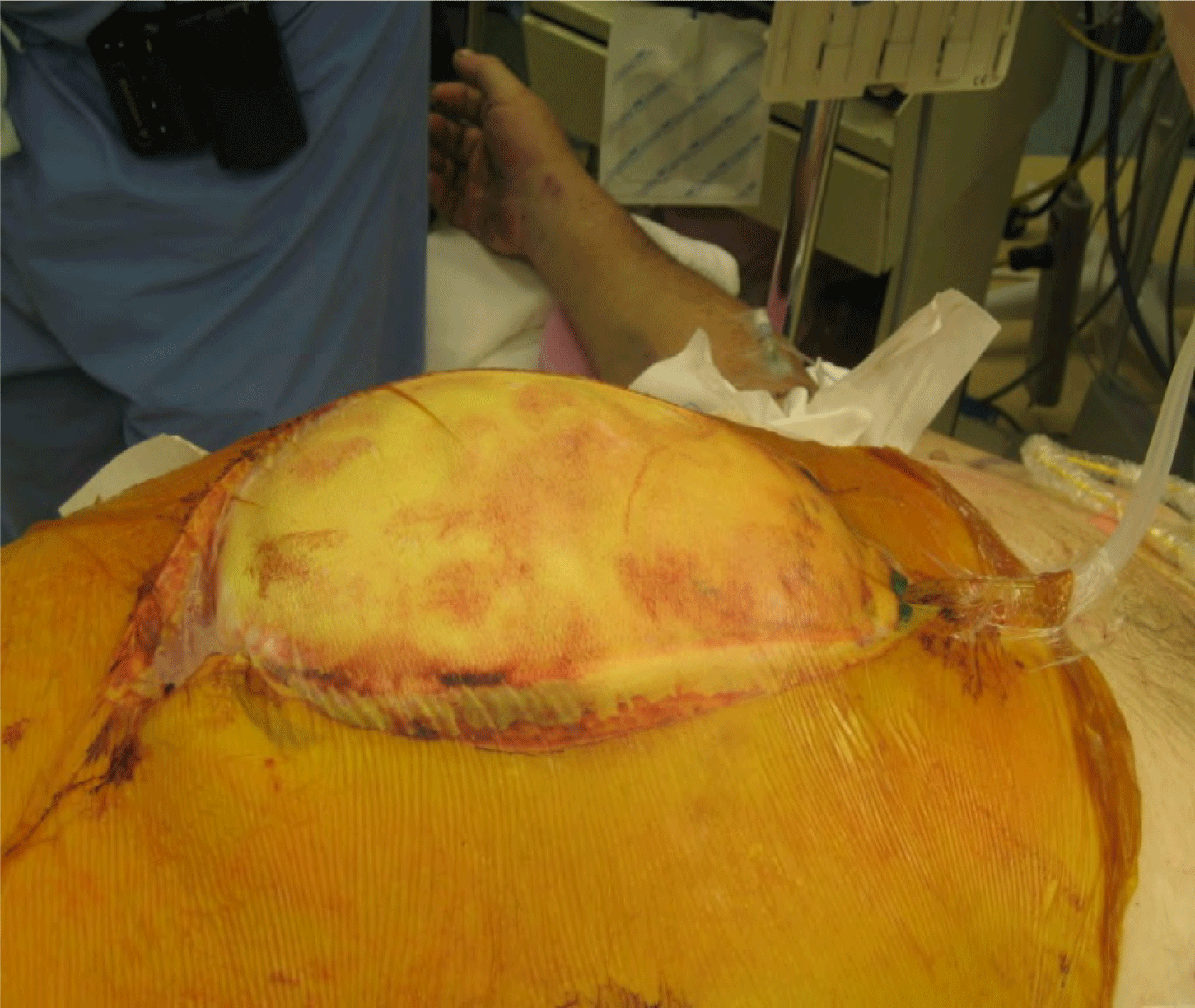
- Any patient with risk factors for developing abdominal hypertension should have intra-abdominal pressure assessed, preferably via intermittent or continuous transbladder pressure.
- Patients diagnosed with abdominal compartment syndrome require emergent decompressive laparotomy and the creation of a temporary abdominal closure.
Latest Updates


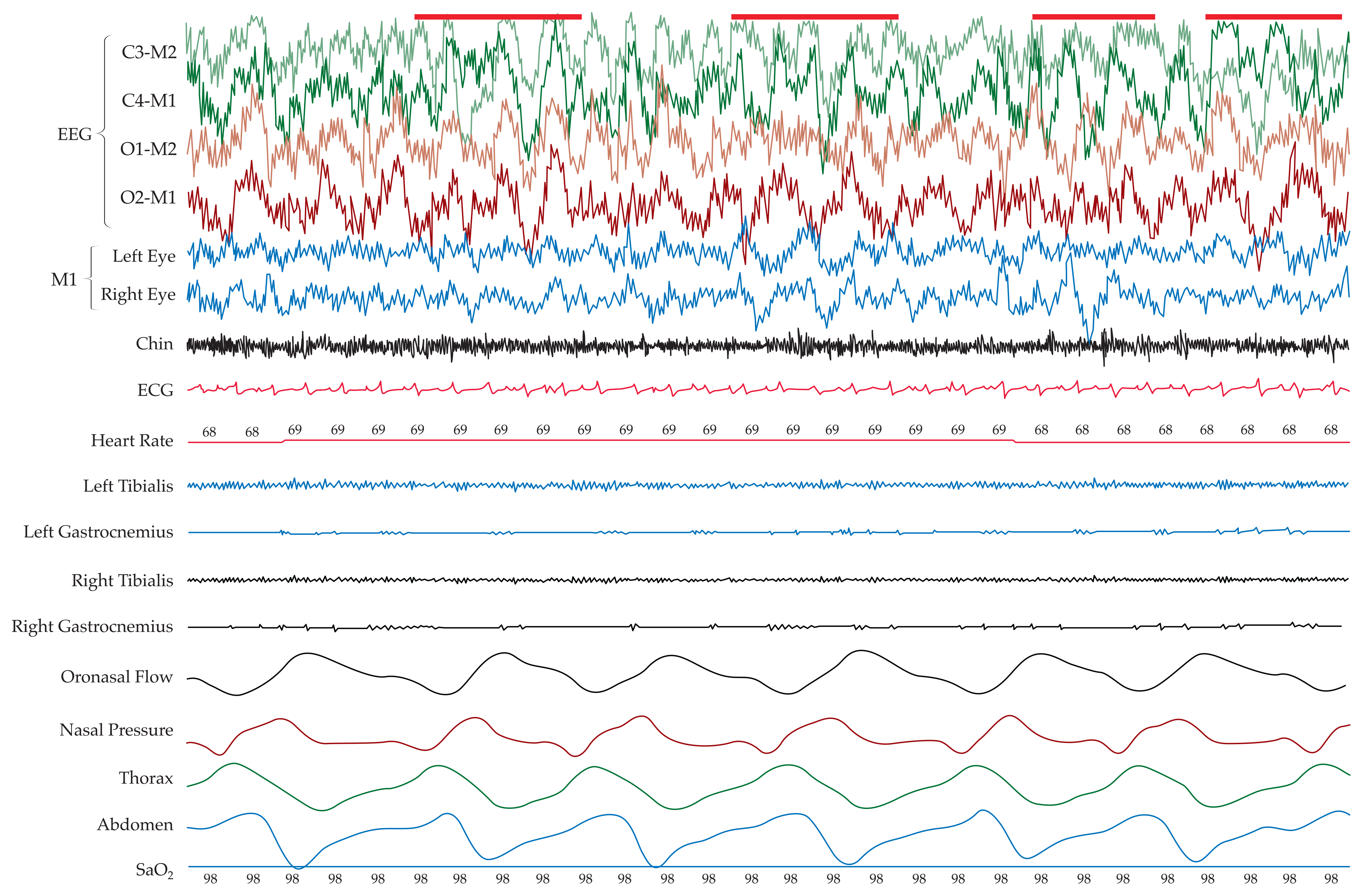
- The MSLT is essential in documenting pathologic sleepiness (e.g., sleep-onset latency of less than 8 minutes) and in diagnosing narcolepsy. The presence of two sleep-onset REMs on four or five nap studies and sleep-onset latency of less than 8 minutes strongly suggests a diagnosis of narcolepsy in the context of an appropriate history.
- RLS is a lifelong sensorimotor neurologic disorder with a severe impact on sleep and quality of life that may begin at any age. RLS is most severe in middle-aged or elderly persons, in whom it has a chronic, progressive course. The overall prevalence of RLS for the adult population has been estimated to be about 7.2%, particularly in those of European descent, but the prevalence of the most severe cases (severe symptoms occurring at least two nights a week) is approximately 2.7%
- For transient insomnia or insomnia of short duration, treatment with sedative-hypnotics (e.g., zolpidem, zolpidem extended release, zolpidem tartrate sublingual tablets, zaleplon, eszopiclone, or low-dose doxepin) or short- or intermediate-acting benzodiazepines (e.g., temazepam), as well as ramelteon, a melatonin receptor (MT1 and MT3) agonist, for a few nights to a few weeks is appropriate.

- The MSLT is essential in documenting pathologic sleepiness (e.g., sleep-onset latency of less than 8 minutes) and in diagnosing narcolepsy. The presence of two sleep-onset REMs on four or five nap studies and sleep-onset latency of less than 8 minutes strongly suggests a diagnosis of narcolepsy in the context of an appropriate history.
- RLS is a lifelong sensorimotor neurologic disorder with a severe impact on sleep and quality of life that may begin at any age. RLS is most severe in middle-aged or elderly persons, in whom it has a chronic, progressive course. The overall prevalence of RLS for the adult population has been estimated to be about 7.2%, particularly in those of European descent, but the prevalence of the most severe cases (severe symptoms occurring at least two nights a week) is approximately 2.7%
- For transient insomnia or insomnia of short duration, treatment with sedative-hypnotics (e.g., zolpidem, zolpidem extended release, zolpidem tartrate sublingual tablets, zaleplon, eszopiclone, or low-dose doxepin) or short- or intermediate-acting benzodiazepines (e.g., temazepam), as well as ramelteon, a melatonin receptor (MT1 and MT3) agonist, for a few nights to a few weeks is appropriate.

- The MSLT is essential in documenting pathologic sleepiness (e.g., sleep-onset latency of less than 8 minutes) and in diagnosing narcolepsy. The presence of two sleep-onset REMs on four or five nap studies and sleep-onset latency of less than 8 minutes strongly suggests a diagnosis of narcolepsy in the context of an appropriate history.
- RLS is a lifelong sensorimotor neurologic disorder with a severe impact on sleep and quality of life that may begin at any age. RLS is most severe in middle-aged or elderly persons, in whom it has a chronic, progressive course. The overall prevalence of RLS for the adult population has been estimated to be about 7.2%, particularly in those of European descent, but the prevalence of the most severe cases (severe symptoms occurring at least two nights a week) is approximately 2.7%
- For transient insomnia or insomnia of short duration, treatment with sedative-hypnotics (e.g., zolpidem, zolpidem extended release, zolpidem tartrate sublingual tablets, zaleplon, eszopiclone, or low-dose doxepin) or short- or intermediate-acting benzodiazepines (e.g., temazepam), as well as ramelteon, a melatonin receptor (MT1 and MT3) agonist, for a few nights to a few weeks is appropriate.
- When massive bleeding exists and direct control of the site of bleeding is under way, the decision to transfuse should be based primarily on hemodynamic status rather than on the hemoglobin or hematocrit level. These laboratory values do not reflect acute hemorrhage because there is a time lag before these levels equilibrate from fluid shift between the extravascular and vascular compartments and from administration of IV fluids.
- The concept of liberal, early use of plasma and platelets developed in large part from the recent US-led military campaigns in Iraq and Afghanistan. Initially in those conflicts, the lack of a reliable supply of blood products near the scene of injury—and platelets especially—led to the use of fresh whole blood transfusion. Although fresh whole blood would be impractical in the civilian setting because of logistical issues and the risk of transmitting transfusion-related infections, the perception of improved outcomes associated with its use prompted military surgeons to advocate 1:1:1 transfusion.
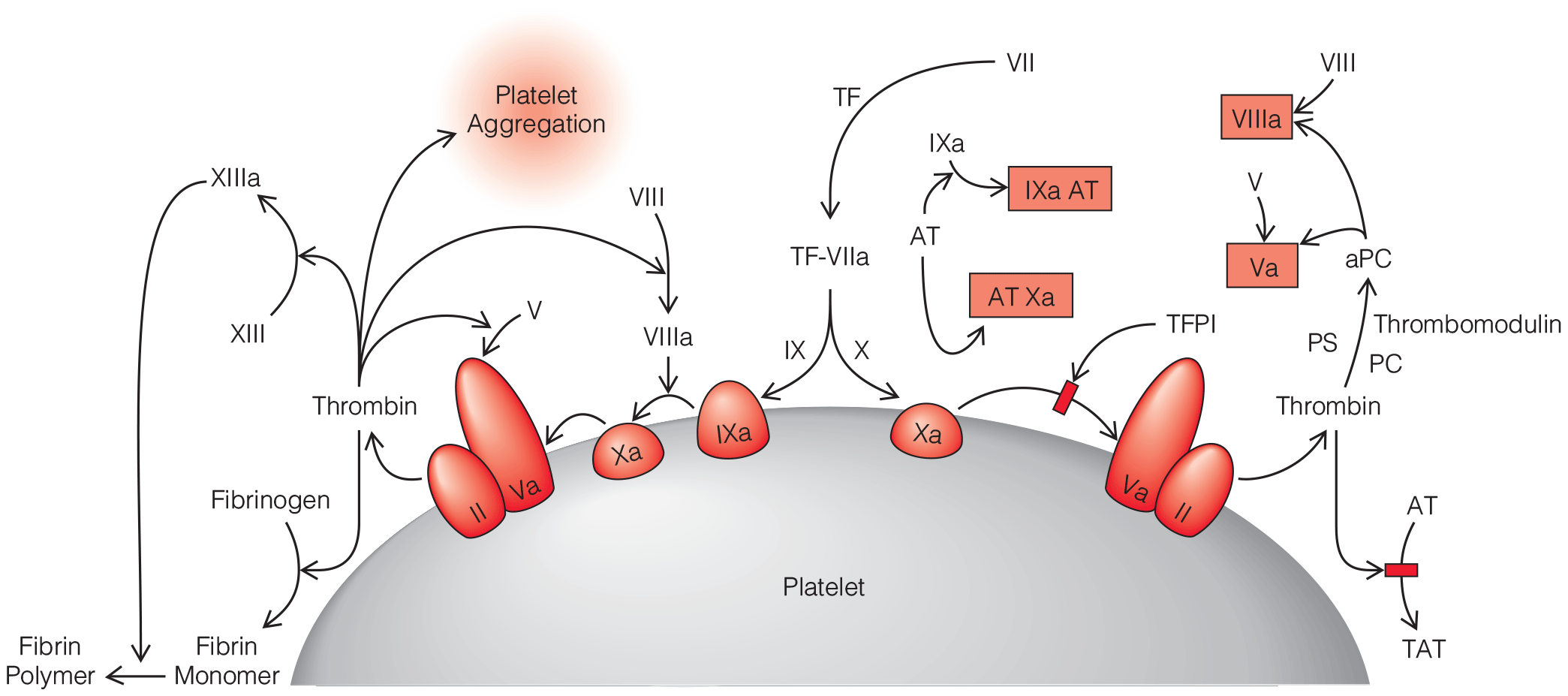
- Beyond recognition and correction of the underlying problem causing DIC and the associated coagulopathy, the diagnosis of DIC represents something of an academic exercise because there is no specific treatment for the condition. Scoring systems that assess the severity of DIC are most useful for distinguishing DIC from other causes of coagulopathy (e.g., hypothermia, dilution, and drug effects).
- When massive bleeding exists and direct control of the site of bleeding is under way, the decision to transfuse should be based primarily on hemodynamic status rather than on the hemoglobin or hematocrit level. These laboratory values do not reflect acute hemorrhage because there is a time lag before these levels equilibrate from fluid shift between the extravascular and vascular compartments and from administration of IV fluids.
- The concept of liberal, early use of plasma and platelets developed in large part from the recent US-led military campaigns in Iraq and Afghanistan. Initially in those conflicts, the lack of a reliable supply of blood products near the scene of injury—and platelets especially—led to the use of fresh whole blood transfusion. Although fresh whole blood would be impractical in the civilian setting because of logistical issues and the risk of transmitting transfusion-related infections, the perception of improved outcomes associated with its use prompted military surgeons to advocate 1:1:1 transfusion.
- Beyond recognition and correction of the underlying problem causing DIC and the associated coagulopathy, the diagnosis of DIC represents something of an academic exercise because there is no specific treatment for the condition. Scoring systems that assess the severity of DIC are most useful for distinguishing DIC from other causes of coagulopathy (e.g., hypothermia, dilution, and drug effects).

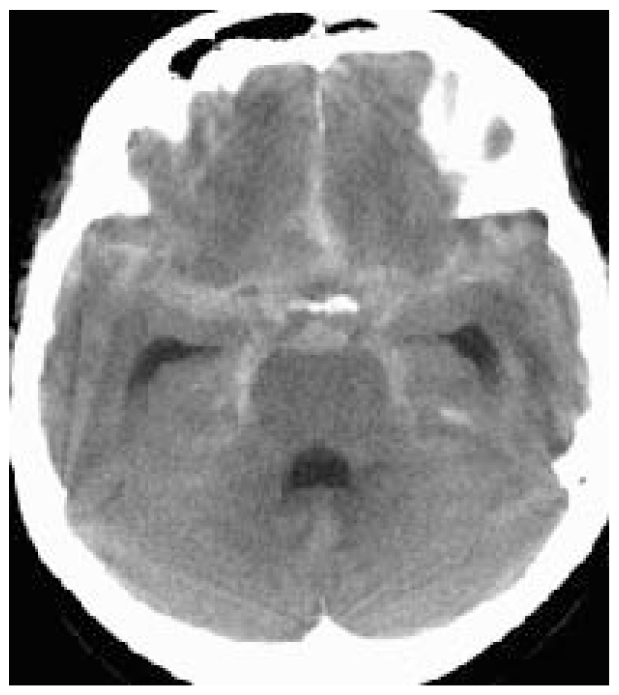
- Computed tomographic angiography (CTA) has the advantage of being noninvasive, but there are very limited data to compare a CTA approach with the current standard diagnostic approach. A methodological review supported CTA in patients presenting within 48 hours of symptoms and with a neurologically intact examination. CTA has not replaced the current approach but has gained more acceptance; its use is center specific and more prevalent in continued management than initial diagnosis. CTA sensitivity decreases with aneurysms less than 4 mm in size and carries the risk of contrast-induced nephropathy, especially if digital subtraction angiography is performed after CTA.
- Current data suggest that very short courses of antifibrinolytics may reduce rebleeding without causing ischemia. Rapid diagnosis of SAH and early definitive repair probably remain the best strategy for prevention. Fibrinolytics should be used in consultation with the neurosurgeon and may be most beneficial in instances of delayed definitive repair.
- The mortality from aSAH appears to have declined in industrialized nations over the past 25 years. The case-fatality rate for aSAH, although still high worldwide, appears globally to be minimally on the decline despite significant regional differences in reporting of mortality.
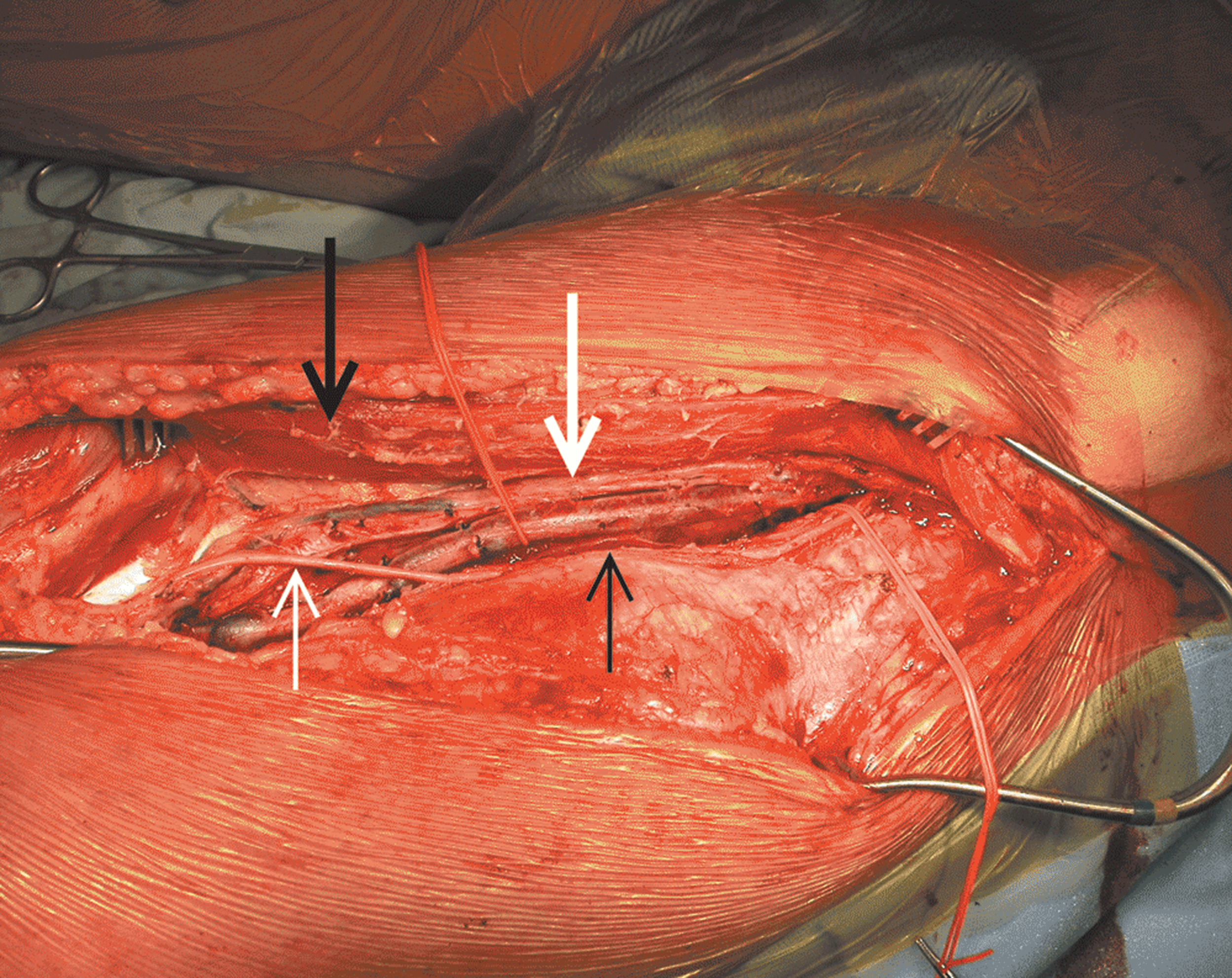
Surgical Treatment of the Infected Aortic Graft
- Discussion of the management of aortic endograft infections, which are increasing in incidence and prevalence and represent a particularly technically challenging subset of aortic graft infections (AGIs)
- Discussion of the management of aortoenteric fistula, with special attention paid to the disastrous effects of gastrointestinal complications
- Updated review of the various methods of arterial reconstruction for AGI, with updated summary of outcomes







.png)