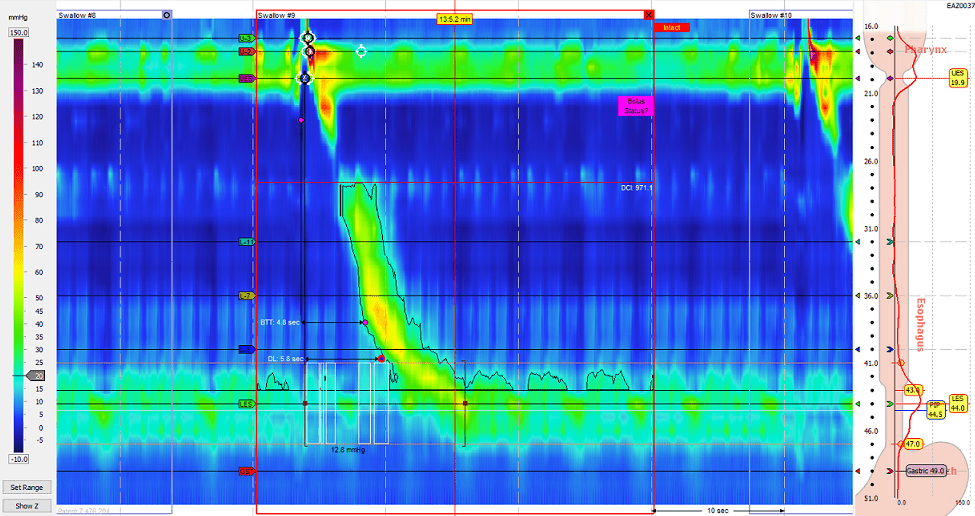
- High resolution manometry: A technology that facilitates topographic evaluation of esophageal motility.
- Wireless pH monitoring: A technique for pH monitoring that does not require an in-dwelling catheter, thought it requires endoscopic placement and does not provide impedance information
- Eosinophilic Esophagitis: A diagnosis of increasing frequency that causes dysphagia in pediatric and adult populations
- Transnasal esophagoscopy: A methodology for esophagoscopy that facilitates evaluation of the pharynx, larynx and pharyngoesophageal segment in contrast to traditional transoral esophagoscopy. Additionally, this can be done in office without sedation.
Latest Updates

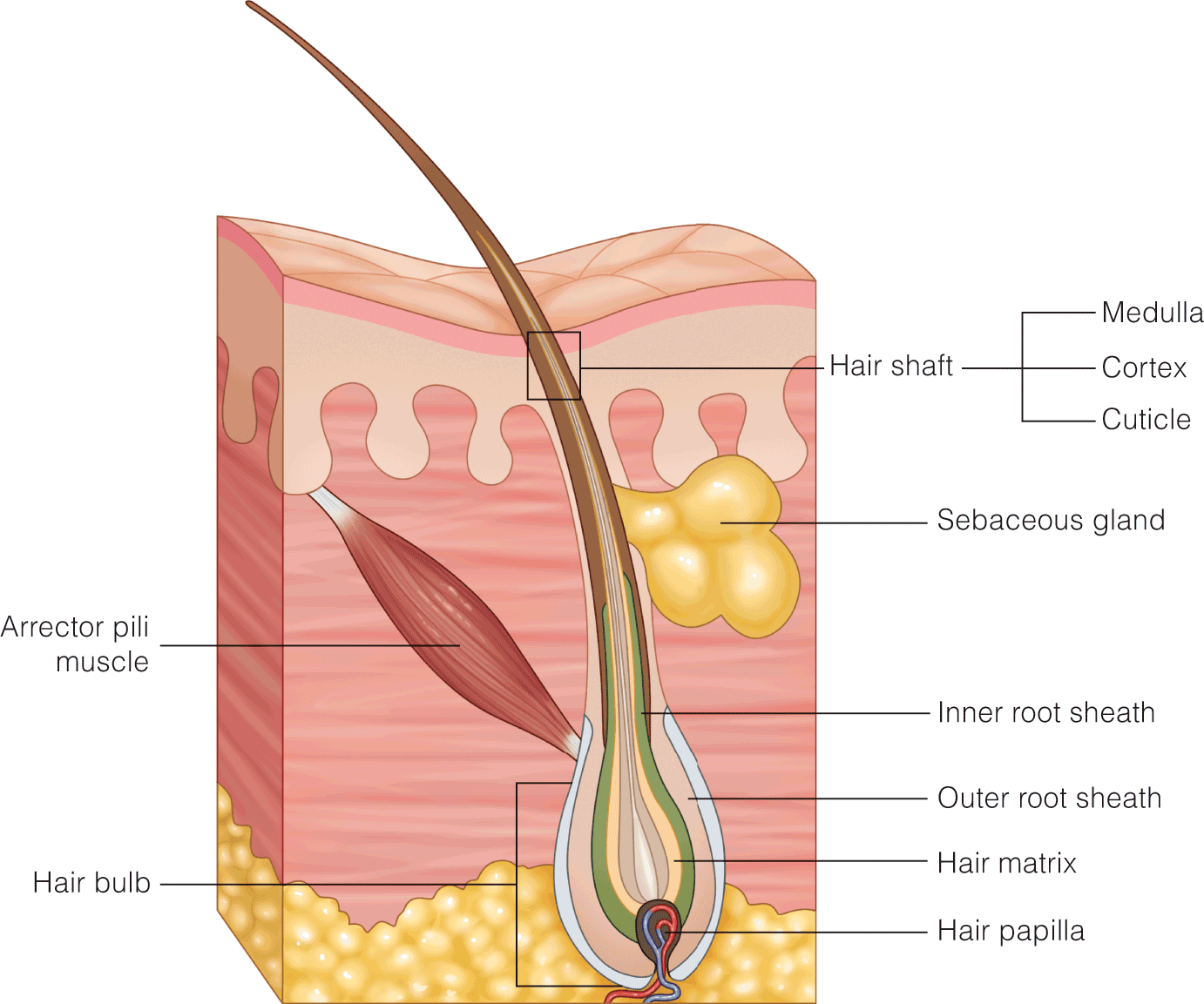
- Robot assisted hair transplantation: Robotic follicular unit extraction is a technique that is gaining popularity to more quickly and accurately harvest follicular units for transplantation.
- Novel drug treatments for hair loss: There are multiple novel drug treatments being developed and studied that have the potential to revolutionize hair loss treatment.
- Adjuvant therapies: Adjuvant treatments such as platelet-rich plasma, lasers, and stem cells have shown some benefit for hair loss.
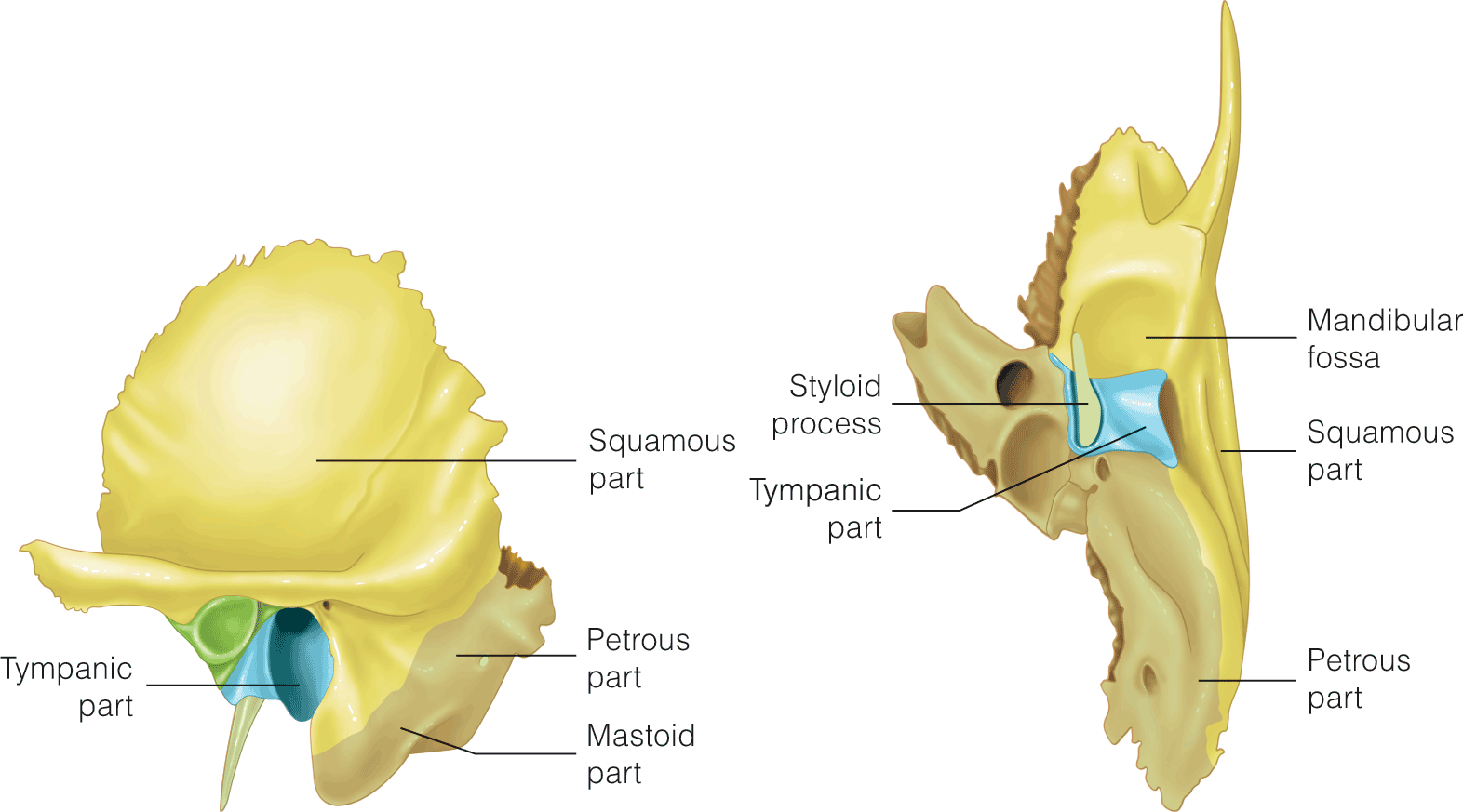
Middle/Inner Ear and Temporal Bone trauma
- The otic capsule violating versus otic capsule sparing classification system of temporal bone trauma has been gaining traction
- While typical protocols rely on a single EnOG facial nerve study between 3-14 days following the injury, serial ENoG may offer additional clinical information to guide surgical decision making in facial nerve palsy beyond two weeks after temporal bone trauma.
- The role of facial nerve decompression following temporal bone trauma remains an area of active inquiry with data in the literature reporting both promising outcomes and outcomes worse than control following surgical intervention.
- There is emerging interest in the use of endoscopic techniques in surgical facial nerve decompression for temporal bone trauma.
- The use of cochlear implantation to treat posttraumatic sensorineural hearing loss among patients who meet audiologic implant criteria is supported by the literature in temporal bone fractures with or without involvement of the otic capsule, as well as in cases of otic concussion without fracture.

- Computed tomographic angiography (CTA) has the advantage of being noninvasive, but there are very limited data to compare a CTA approach with the current standard diagnostic approach. A methodological review supported CTA in patients presenting within 48 hours of symptoms and with a neurologically intact examination. CTA has not replaced the current approach but has gained more acceptance; its use is center specific and more prevalent in continued management than initial diagnosis. CTA sensitivity decreases with aneurysms less than 4 mm in size and carries the risk of contrast-induced nephropathy, especially if digital subtraction angiography is performed after CTA.
- Current data suggest that very short courses of antifibrinolytics may reduce rebleeding without causing ischemia. Rapid diagnosis of SAH and early definitive repair probably remain the best strategy for prevention. Fibrinolytics should be used in consultation with the neurosurgeon and may be most beneficial in instances of delayed definitive repair.
- The mortality from aSAH appears to have declined in industrialized nations over the past 25 years. The case-fatality rate for aSAH, although still high worldwide, appears globally to be minimally on the decline despite significant regional differences in reporting of mortality.

Management of Complicated Gallstone Disease
- Laparoscopic cholecystectomy is one of the most frequently performed operations in the United States, with nearly 800,000 cholecystectomies performed annually. The laparoscopic cholecystectomy is an intriguing operation because of its perception as a technically simple procedure.
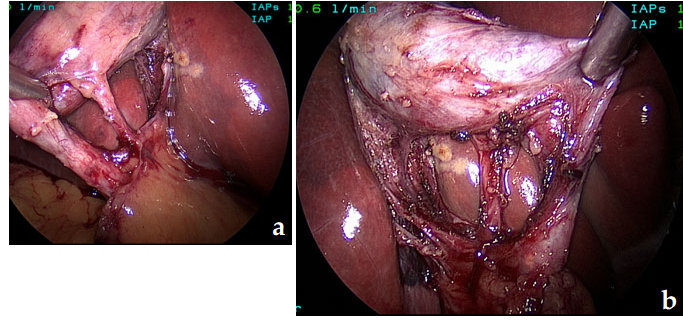
- Although the goal is to always obtain the critical view of safety and perform a cholecystectomy, there are instances (increased inflammation, fused structures, and variant anatomy) in which this view cannot safely be obtained. In the setting of chronic inflammation, structures contract and fuse together, often obliterating clear planes between different structures.
- There are myriad causes of pancreatitis such as alcohol and trauma, but one common cause is gallstones, which is believed to cause up to 60% of the cases of pancreatitis.

Management of Complicated Gallstone Disease
- Laparoscopic cholecystectomy is one of the most frequently performed operations in the United States, with nearly 800,000 cholecystectomies performed annually. The laparoscopic cholecystectomy is an intriguing operation because of its perception as a technically simple procedure.
- Although the goal is to always obtain the critical view of safety and perform a cholecystectomy, there are instances (increased inflammation, fused structures, and variant anatomy) in which this view cannot safely be obtained. In the setting of chronic inflammation, structures contract and fuse together, often obliterating clear planes between different structures.
- There are myriad causes of pancreatitis such as alcohol and trauma, but one common cause is gallstones, which is believed to cause up to 60% of the cases of pancreatitis.
- Computed tomographic angiography (CTA) has the advantage of being noninvasive, but there are very limited data to compare a CTA approach with the current standard diagnostic approach. A methodological review supported CTA in patients presenting within 48 hours of symptoms and with a neurologically intact examination. CTA has not replaced the current approach but has gained more acceptance; its use is center specific and more prevalent in continued management than initial diagnosis. CTA sensitivity decreases with aneurysms less than 4 mm in size and carries the risk of contrast-induced nephropathy, especially if digital subtraction angiography is performed after CTA.
- Current data suggest that very short courses of antifibrinolytics may reduce rebleeding without causing ischemia. Rapid diagnosis of SAH and early definitive repair probably remain the best strategy for prevention. Fibrinolytics should be used in consultation with the neurosurgeon and may be most beneficial in instances of delayed definitive repair.
- The mortality from aSAH appears to have declined in industrialized nations over the past 25 years. The case-fatality rate for aSAH, although still high worldwide, appears globally to be minimally on the decline despite significant regional differences in reporting of mortality.


Epilepsy and Related Disorders
- Brain imaging has made significant progress in recent years and is a cornerstone of diagnosis and characterization of epilepsy.
- The diagnosis and management of psychogenic non-epileptic seizures has significantly evolved in recent years.
- Current practice is to use the drug as monotherapy. The dose is progressively increased until seizures are controlled or adverse effects develop. If seizure control cannot be achieved without significant adverse effects, the drug is considered a failure, and a second drug is chosen and the process is repeated. If the second drug fails, either a third monotherapy trial or a combination therapy can be attempted.









.png)